This content includes a lot of grammatical and vocabulary errors.Please cut me some slack from Japan.
This article deals with “Cubital Tunnel Syndrome,” in which the ulnar nerve is affected at the elbow.
Symptoms include motor and sensory neuropathy, and motor disorders include clumsiness in the fingers and difficulty in bending and extending the little finger and ring finger. Sensory deficits include decreased sensation and numbness of the little finger to the ring finger and the little finger side of the palm of the hand.
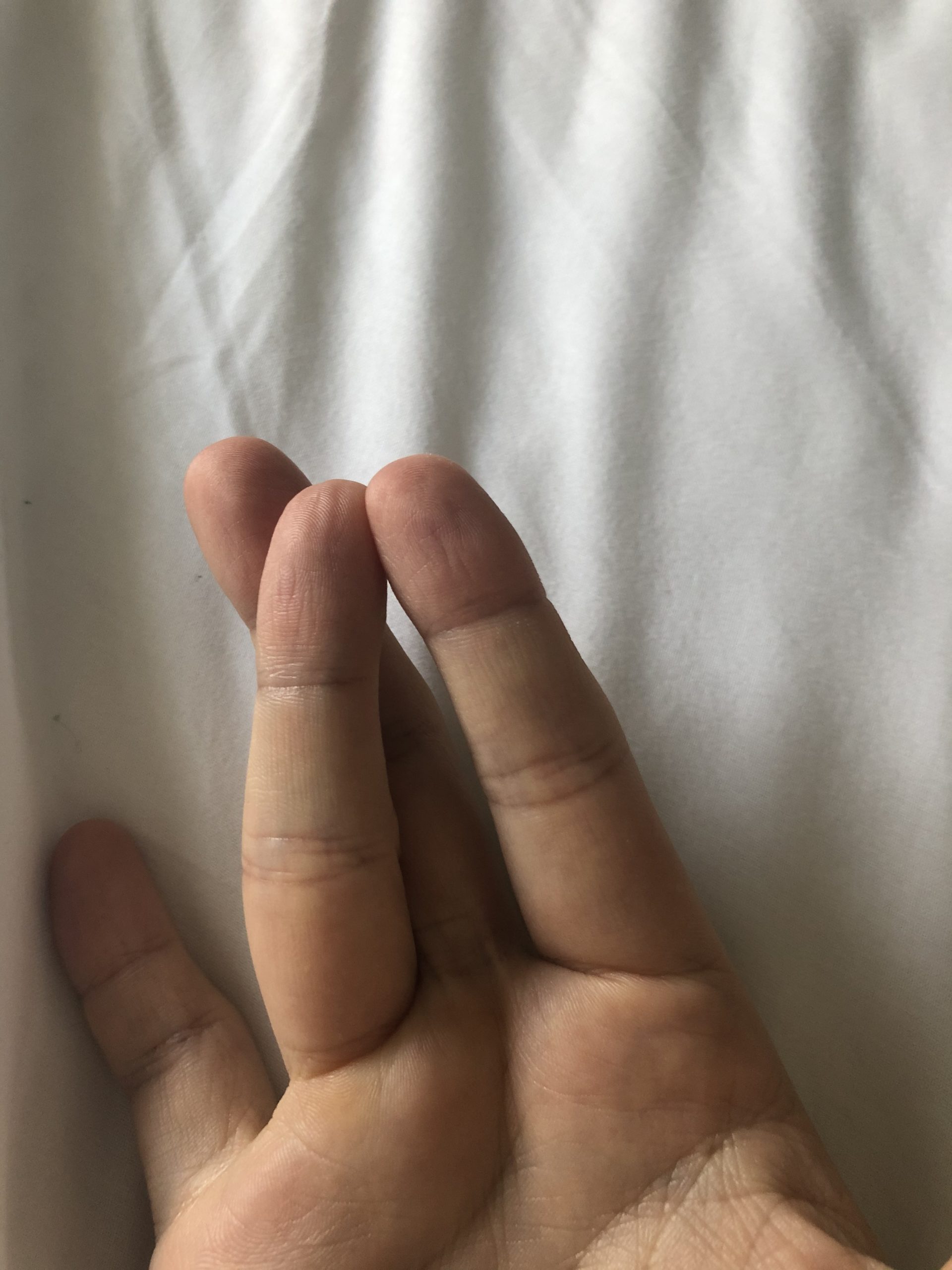
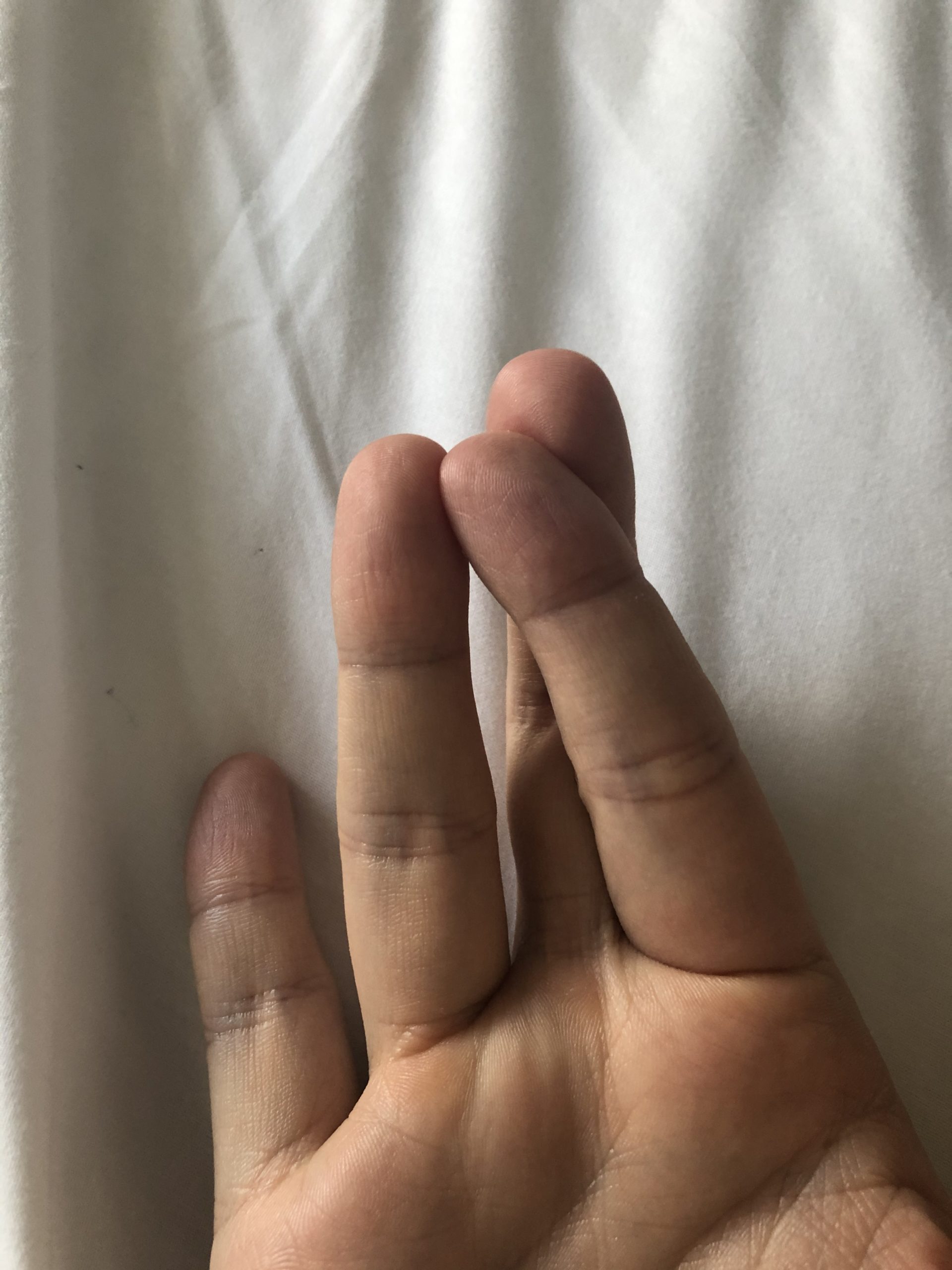
There are various tests for motor disorders, but the middle finger internal/external rotation test seems to be the easiest to understand. As shown in the figure below, the middle finger is rolled inward and outward over the ring finger.
The most important aspect of the sensory disturbance is that there is no hypoesthesia or numbness on the ulnar (medial) side of the forearm. The ulnar aspect of the forearm is not affected by cubital tunnel syndrome because it is a nerve derived from the brachial plexus called the medial antebrachial cutaneous nerve. If the ulnar aspect of the forearm is affected, brachial plexus or spinal cord disease is suspected.
Nerve Conduction Test
The following nerves are examined
(1) Ulnar nerve (motor and sensory nerves)
(2) Median nerve (motor and sensory nerve) Auxiliary diagnosis
The ulnar nerve is absolutely examined. The elbow joint should be flexed 90 or 135 degrees at that time. The ulnar nerve is loose at the elbow joint 0 degrees (elbow extension) ≈ measurement error is likely to occur when measuring distance, so the elbow is flexed to apply a little tension.
In addition, the “inching method” is often used for cubital tunnel syndrome. Inching is a technique to stimulate the ulnar nerve every 30 mm (inch) to get an approximate idea of the site of injury.
The reference point is the elbow (the straight line between the olecranon and medial epicondyle on the electromyogram), from which stimulation is applied distally at 30 mm (BE30 Below Elbow) and proximally at 3/6/9 cm (AE30, AE60, AE90 Above Elbow). We see where the conduction velocity (NCV Neuron Conduction Velocity) drops.

There are some diagnostic criteria for cubital tunnel syndrome.
(1) NCV of AE-BE < 50 m/s
(2) NCV of AE-BE is 10m/s or more lower than that of BE-Wrist
(3) Amplitude (height of potential CMAP) of AE is 20% or more lower than that of BE
(4) The shape of the waveform is different between AE and BE stimulation
When at least two of (1)-(4) are satisfied, cubital tunnel syndrome is diagnosed. Please keep this in mind. The criteria for (4) are a little vague, though.
The sensory nerve SNAP is measured, but does not specifically affect the elbow syndrome diagnostic criteria.
The median nerve is used to rule out peripheral neuropathies other than elbow pain syndrome (diabetes, anticancer drugs, nerve disease), brachial plexus disorders, cervical myelopathy, etc. It is recommended to perform the EMG of the ulnar nerve, but sometimes the needle EMG (APB: abductor pollicis brevis) described below can be used as a substitute.
The F wave of the ulnar nerve does not need to be measured in elbow syndrome. It is not necessary to measure the F wave of the ulnar nerve in elbow canal syndrome, because it is absolutely abnormal and there is no point in measuring it even if it causes pain.
Guyon’s canal syndrome is easily mistaken for cubital tunnel syndrome.
Guyon’s canal syndrome is a condition similar to elbow canal syndrome.
The ulnar nerve is injured at the elbow in elbow duct syndrome, whereas it is injured at the wrist in Guyon’s duct syndrome. For more information, please refer to the “Link: Gyuon’s canal syndrome.
The points are
(1) Ulnar nerve CMAP0SNAP× (ADM〇 FDI×)
SNAP of the dorsal hand branch of the ulnar nerve is normal.
The point is that there is a dissociation between CMAP and SNAP.
Needle EMG
Muscles to be stung absolutely: FDI (short thumb abductor muscle) FCU (ulnar carpometacarpal flexor muscle)
Almost always prick muscle: APB (short thumb abductor muscle)
The FDI and FCU are always pricked to compare the two findings: the FDI is the most distal muscle innervated by the ulnar nerve, while the FCU is not affected in cubital tunnel syndrome because the ulnar nerve branches before it enters the elbow tube. This anatomic reason confirms that the FCU is normal. In summary, FDI x FCU 〇 for elbow duct syndrome. If FDI x FCU x, ulnar neuropathy, brachial plexus palsy, or spinal cord disease other than cubital tunnel syndrome is suspected.
Other muscles do not sting much. In fact, there are not many muscles that can be examined for C8 and Th1 dominance, and other than FDI/FCU/APB, the only muscles that can be examined are the EIP/erect spinal muscles.
In summary
FDI x APB 〇 FCU 〇
⇒cubital tunnel syndrome
FDI x APB 〇 FCU x
⇒ Ulnar neuropathy, brachial plexus palsy, spinal cord disease (however, only C8 is particularly affected, so the frequency is quite low)
FDI×APB×FCU×⇒Brachial plexus palsy, Brachial plexus palsy, Spinal cord disease
⇒ Brachial plexus palsy, spinal cord disease (this is more likely to occur than the above)
The examination will be performed with attention to the inching method, dissociation of FDI and FCU findings, etc.
That is all. Thank you again.