This content includes a lot of grammatical and vocabulary errors.Please cut me some slack from Japan.
This section is about “Carpal Tunnel Syndrome,” the most common disease among those who undergo electromyography.
Summary
CMAP Distal latency>4.4ms
2L-int/Ring latency difference >0.5 ms, respectively
Carpal tunnel syndrome = median nerve palsy
Carpal tunnel syndrome is a typical disease in which the median nerve is paralyzed, resulting in loss of hand function and sensation. The most common symptoms are (1) dull and numb sensation in the thumb to ring finger and (2) difficulty in moving the fingers. In particular, (2) is often noticed when buttoning clothes or using clothespins. These are caused by damage to the median nerve.
Let’s take a look at what is actually examined.
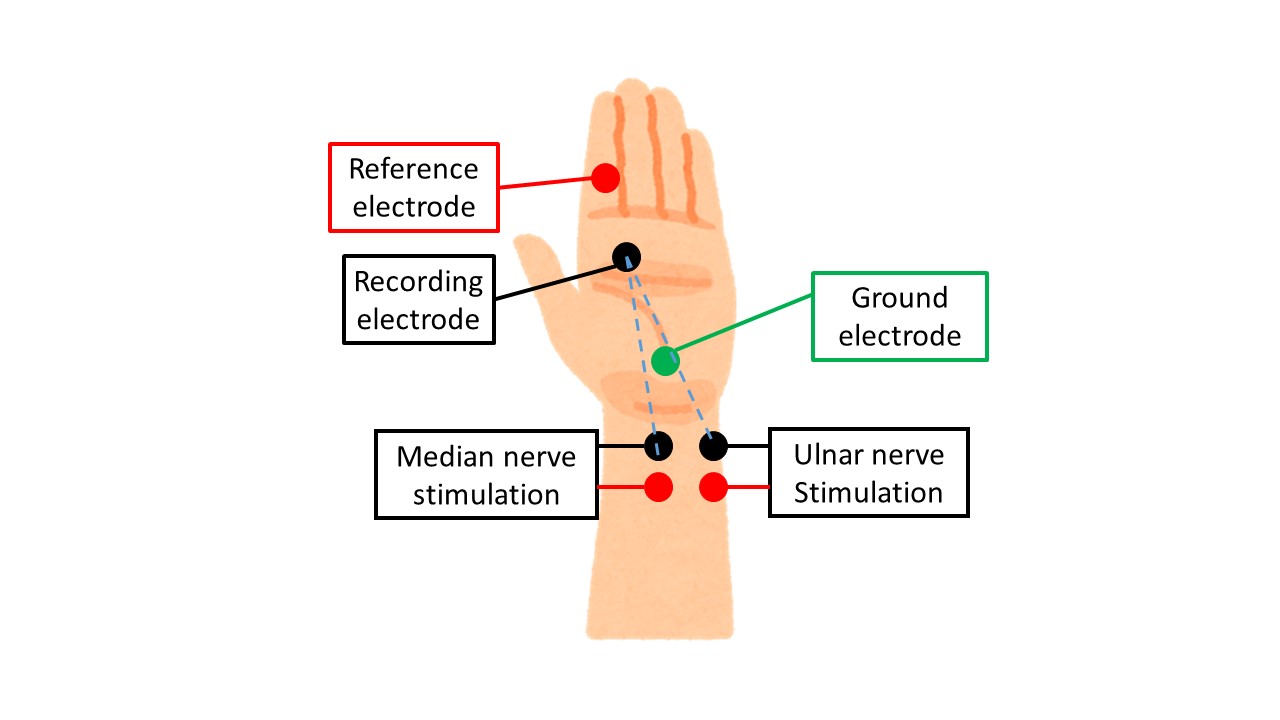
Nerve Conduction Test
In evoked electromyography, we will do the following
(1) Median nerve (motor and sensory nerves) Absolutely
(2) Ulnar nerve (motor and sensory nerve) Auxiliary diagnosis
The median nerve is absolutely examined first.
In carpal tunnel syndrome, the minimum latency of CMAP (Compound Muscle Action Potentials) during stimulation at the wrist is particularly important. The minimum latency is the shortest time from electrical stimulation to CMAP, and if it is 4.4 ms or longer, carpal tunnel syndrome is suspected.
The time difference between elbow stimulation and wrist stimulation is used to determine the nerve conduction velocity (NCV: Neuro conduction velocity), which is normal or slightly decreased in pure carpal tunnel syndrome. This is because in carpal tunnel syndrome, the median nerve is injured in the wrist joint, and the nerve from the elbow to the wrist joint is often normal. (However, if dying-back occurs, in which the nerve degenerates from the periphery, the value will be abnormal.
Sensory nerves in the median nerve are often slowed down, reduced in size, or not present at all. This is because sensory nerves are thinner than motor nerves and thus are affected earlier, and the sensory nerve waveform SNAP (Sensory Nerve Action Potentials) is very small (1/1000th of CMAP), so it is difficult to distinguish it from noise.
The ulnar nerve is used to rule out peripheral neuropathies other than carpal tunnel syndrome (diabetes, anticancer drugs, nerve disease), brachial plexus disorders, cervical myelopathy, etc. It is sometimes substituted with needle electromyography (FDI: first dorsal interosseous muscle) as described below, although it is better to perform it.
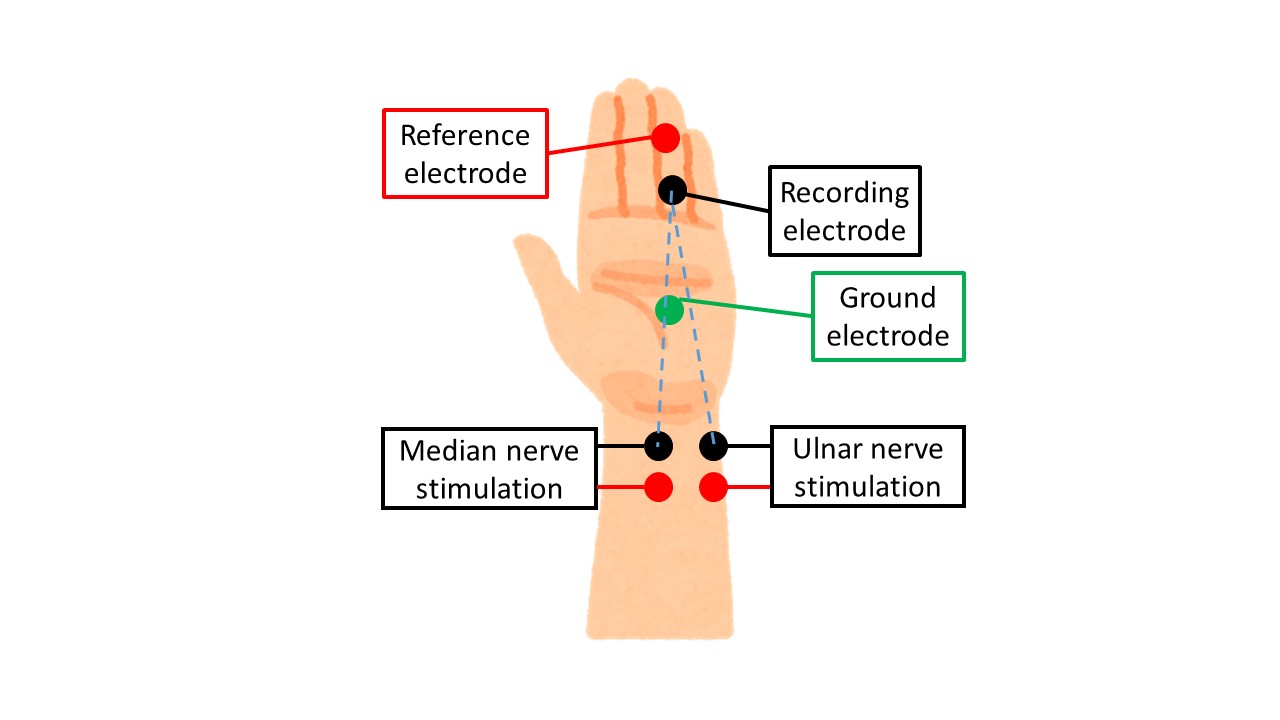
Comparison test
A comparison test is often performed as a bonus to the nerve conduction study.
This is based on the median nerve x ulnar nerve 〇 , nature of carpal tunnel syndrome, and typical examples are the most common types of comparison tests are (1) 2L-Int (motor nerve) and (2) ring finger comparison method (sensory nerve).
2L-Int
The 2L-Int refers to the second and palmar interosseous muscles, which are innervated by the median nerve and the ulnar nerve, respectively. Since these muscles are adjacent to each other and similar waveforms can be read by the recording electrode during electrical stimulation, we use this property to compare the minimum latency difference during stimulation of the median and ulnar nerves from the same distance (12-14 cm).
If the minimum latency during stimulation of the median nerve is slower than 0.5 ms, carpal tunnel syndrome is diagnosed.
As a side note, the usual median nerve CMAP is measured in the APB (abductor pollicis brevis) muscle, which is prone to early damage and often fails to show a waveform in the test. However, the 2L-Int is more easily spared than the APB, making it a very valuable test in patients with atrophied APB.
Ring finger comparison method
As those who have studied anatomy know, the sensation in the ring finger is innervated by the median nerve on the flexor side and the ulnar nerve on the ulnar side. Therefore, the minimum latency difference between stimulation of the median and ulnar nerves from the same distance (10-12 cm) with electrodes attached to the ring finger is compared, and if the minimum latency of stimulation of the median nerve is slower than 0.5 ms, carpal tunnel syndrome is diagnosed.
Needle electromyography
Needle electromyography examines the following
(1) Absolute stabbing muscle: APB (short thumb abductor muscle)
(2) Almost always stabbing muscle: FDI (first dorsal interosseous muscle)
(3) Muscles to be occasionally stung: C6, 7, 8 muscles, Paraspinal
The APB and FDI are almost always inserted, since the APB is the most distal muscle innervating the median nerve and the FDI is the most distal muscle innervating the ulnar nerve, so we examine them based on the principle that if they are normal, their innervation as a whole is not impaired. The APB and FDI are also referred to as couple muscles, and since they share the same nerve height (C8, Th1), the difference in findings between the two muscles is examined to rule out spinal cord or spinal cord lesions. In carpal tunnel syndrome, this would be APB x FDI0.
If the above APB x FDI 〇 is found, the examination is almost finished there. However, to examine the muscles innervated by the median nerve in detail, we look at the APB distal to the wrist joint and the FCR (flexor carpi radialis flexor) and PT (piriformis teres) proximal to the wrist joint, depending on the patient’s mood. Other muscles to examine are C6, 7, and 8, selected from the areas with the strongest sensory disturbance. For example, if the middle finger (middle toe) is very symptomatic, I will look at the C7 triceps muscle. If they are normal, the suspicion of carpal tunnel syndrome is increased.
When APB x FDI x (FCR 〇 or PT 〇), the paraspinal (paraspinal erector spinae muscle group) may also be pricked, which is useful in differentiating whether the lesion is a peripheral or central lesion (spinal cord lesion) because the paraspinal is the most recently located muscle. In summary, paraspinal 〇 => peripheral neuropathy or brachial plexus disorder, paraspinal x => spinal cord lesion.
The following is a summary of needle EMG findings and diseases.
APB x FDI 〇 (FCR 〇 or PT 〇)
⇒Carpal tunnel syndrome
APB×FDI〇(FCR× or PT×) ⇒Median nerve palsy or arm
⇒Median nerve palsy or brachial plexus palsy or spinal cord disease
APB×FDI×(FCR×orPT×) Paraspinal0
⇒Peripheral neuropathy or brachial plexus disorder (not so common)
APB×FDI×(FCR〇 or PT〇)Paraspinal×⇒Spinal cord lesion
⇒ Spinal cord lesion
APB×FDI×(FCR×orPT×)
⇒Brachial plexus palsy or spinal cord disease
In this way, we can see if there is only carpal tunnel syndrome or if other factors are involved. The examination itself takes 10-15 minutes for carpal tunnel syndrome alone, or 30 minutes if other factors are involved.
That’s all. Thank you again.