This content includes a lot of grammatical and vocabulary errors.Please cut me some slack from Japan.
This section will be briefly described. Please read the orthography for details.
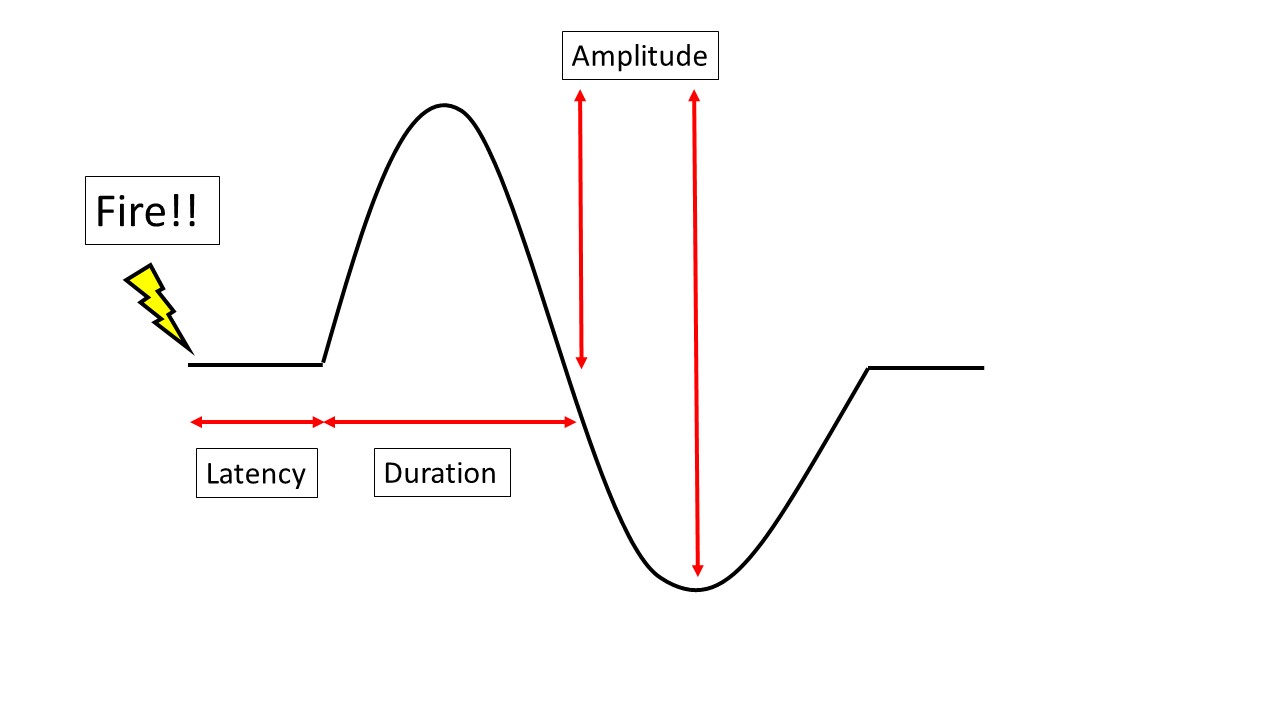
The above y=sinx waveform is the most basic waveform; NCV (nerve conduction velocity), Amplitude (potential), Latency (latency), and Duration (duration) are the important parameters.
NCV (Nerve Conduction Velocity)
NCV stands for Nerve Conduction Velocity. NCV below 50 m/s in the upper extremity and 40 m/s in the lower extremity is considered to be delayed, and “demyelination” is suspected. However, NCV is strongly affected by skin temperature, so be especially careful in winter and in air conditioning.
On the other hand, if it is fast, it does not matter especially if it exceeds 70 m/s in the upper limb and 50 m/s in the lower limb. It is usually just a measurement error.
Amplitude
Amplitude (potential) is said to be abnormal at 10mv in CMAP and 5μv or less in SNAP. However, it is not reliable because there is a large difference between individuals. It is better to look at the difference between left and right, and between upper and lower limbs.
Conduction block” is an important part of Amplitude, and if Amplitude at a certain stimulation site is less than 50~60% of that at the other site or the healthy side, it is considered to be a conduction block. Conduction block is important because it is one of the findings that cause muscle weakness.
Also, if Amplitude is decreased and Duration is prolonged, which will be discussed later, a finding of temporal dispersion can be obtained. This is another finding of conduction block and muscle weakness.
Latency
Latency is particularly important for distal latency, which is obtained by stimulation of the distal portion of the muscle.
Prolonged distal latency is a problem in strangulation disorders, most notably carpal tunnel syndrome and tarsal tunnel syndrome. In the case of carpal tunnel syndrome, the latency is >4.4 ms, and in the case of tarsal tunnel syndrome, the latency is determined by NCV 40 m/s or less, since SNAP is done (Latency = NCV in SNAP, I forgot to mention that).
Distal latency is based on the nerve with the fastest wave rise, which is good if all the nerves are demyelinated, but in reality, demyelination occurs sparsely, so it is important to note that distal latency is not prolonged to the same extent.
Duration
Duration is not judged by itself, but rather the difference between the healthy healthy side and the proximal and distal sides. In particular, the phenomenon of prolonged Duration is called “temporal dispersion. Generally, if the Duration is 20% longer than the proximal Duration during healthy or distal stimulation, it is considered to be temporal dispersion. (Background: Sometimes it is just a formality.)
F wave
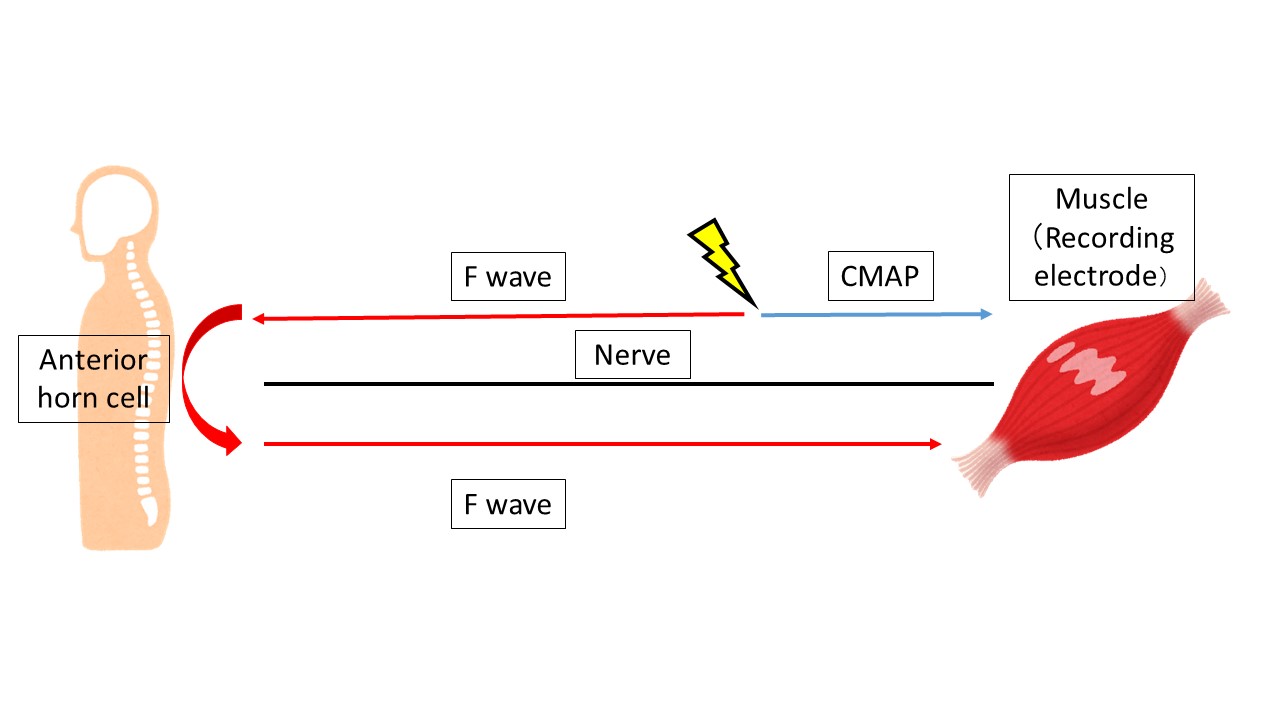
F wave is like a sibling of CMAP. While CMAP travels from the stimulation site to the muscle as described above, the F wave goes to the spinal cord once, makes a U-turn, and then travels to the muscle.
This makes it possible to examine the entire nerve including the spinal cord, making it suitable for detecting systemic pathologies. For example, it is used in Guillain-Barre syndrome and diabetic peripheral neuropathy.
In the F wave, we look at the Minimum Latency (minimum latency) and Frequency (frequency). A minimum latency of 30 for the upper extremity and 40 for the lower extremity is generally considered to be delayed. It is difficult to determine the rate of occurrence because it varies from nerve to nerve, from individual to individual, and depending on the activation of the nerve. It is best to examine both sides and see the difference.
That’s all. Thank you again.