This content includes a lot of grammatical and vocabulary errors.Please never mind from Japan.
One height can make a world of difference.
The detailed movements are described in the manual, so please refer to it. Here, I will describe the key points.
One different spinal cord injury height can drastically change the movements and ADLs (activities of daily living) that can be performed. This is especially true in the cervical cord area.
The notation C5 injury = C5 or higher function remains.
Residual high is defined as MMT≥3 and MM5 in one medullary segment above the MMT. For example, a MMT of C4:5, C5:5, C6:3, and C7:2 indicates a C6 injury. On the other hand, C4:5, C5:4, C6:4, C7:2 would be a C5 injury. Please keep this in mind.
C3 and above
Muscles that move: facial and cervical muscles, trapezius muscles
Since the face and neck can move, it is actually possible to drive the wheelchair by using a machine called “Chin control” that controls the wheelchair with the jaw. However, for safety reasons, the patient is usually accompanied by a chaperone, and basically all ADLs are at the level of full assistance.
The most important aspect in this area is respiratory function.
The diaphragm, the most important part of breathing, is paralyzed by the diaphragmatic nerve (C3-5 C4 main), which controls the diaphragm, resulting in complete or incomplete paralysis. Both inhalation and exhalation are easily impaired, and many patients may not be able to be taken off the ventilator.
However, with proper assessment and planning, 70-80% of C3 and C4 patients can be taken off the ventilator (C2 and above are still difficult).
Typical muscles that can be mobilized: muscles throughout the neck (nothing that will dramatically change movement or ADL).
C4
Typical muscles that can move: diaphragm ⇒ breathing
Since the diaphragm becomes mobile, a ventilator is no longer essential in many cases. However, CPAP may be used to assist breathing only at night (when breathing is generally shallow and arousal rate tends to drop).
As a side note, breathing is basically an inhalation, and as long as you can inhale, you are fine. Exhalation is done by voluntary movement of the rib cage and descending diaphragm, which are inflated by inhalation, so even if paralyzed, the disability is only mild. On the other hand, the diaphragm (diaphragmatic nerve), which is responsible for 70% of inhalation, is the fourth ace in the hole, so paralysis can cause significant disability.
As an added bonus, inhalation is quick due to diaphragmatic contraction, whereas exhalation is a voluntary movement and can only be done slowly. Therefore, the time between inhalation and exhalation is 1:2, with exhalation taking longer.
ADL remains at the full-assistance level.
C5
Typical muscles capable of movement: Deltoid and biceps ⇒ Shoulder joint abduction & flexion, elbow flexion
From this point on, the movements and ADLs that the patient can perform will change considerably.
First of all, the patient will be able to drive a wheelchair on his/her own. However, care must be taken to ensure that the hand rims (wheels used to pedal the wheelchair) are coated with rubber and that leather gloves are worn to increase friction. After bending the elbow, the patient can relax and let gravity rub the leather gloves against the handrims as the elbow is extended, and the friction will propel the wheel forward. However, an elderly person without durability may settle for a power wheelchair without straining.
Many ADLs require assistance, but with BFO (Balanced Forearm Orthosis, MOMO/ Balancer, etc.), patients can perform activities using their upper limbs, such as eating, on their own.
However, dressing, changing, and toileting are difficult.
C6
Typical muscles that can be mobilized: extensor carpi radialis flexors → dorsiflexors of wrist joints
This is the height at which function and ADL change most significantly.
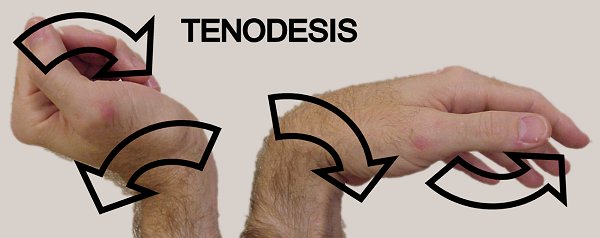
The most important thing is that dorsiflexion of the wrist joint enables “tenodesis” and the ability to grasp objects. Tenodesis is a phenomenon in which the fingers bend when the wrist is turned back, and the fingers extend when the wrist is turned back (see figure below).
Since the strength of the upper limbs is not strong enough with only tenodesis, most of the upper limb functions can be performed with the use of assistive devices. Men can also use self-purge to urinate on their own. This is a very important function that can affect the prognosis of a patient’s life.
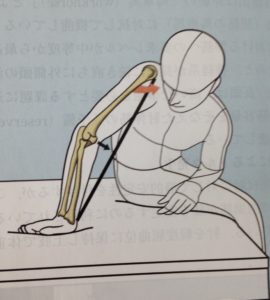
With C6, transfers are also possible.
In this case, the patient dorsiflexes the hand joint and presses it hard against the bed or locks it with a string or bar, while the shoulder joint is horizontally adducted with the pectoralis major muscle and the elbow joint is locked in extension. (The figure below shows the right hand.)

C7
Muscles moved: triceps brachii ⇒ elbow extension, flexor digitorum brevis ⇒ wrist joint palmar flexion, extensor digitorum brevis ⇒ wrist extension
The triceps brachii muscle enables elbow extension, making transfer easier.
In fact, ADL does not change that much from C6, but stability is increased. In addition, women can self-urinate from C7 (although it is also possible in part of C6).
C8/Th1
Typical muscles that become operable: internal hand muscles, wrist joint & finger flexor muscles ⇒ Various movements such as finger flexion and abduction.
Muscles at this height govern the movement of the hand and fingers. With this level of function, most ADLs can be independent and social life can be spent without problems.
Typing can also be done quickly, which will expand the scope of social life and employment for people with disabilities, honestly.
Also, depending on the orthotics (e.g., Prime-Walk Uppall), walking becomes possible at the training level. Stairs are still tough.
L2
Typical muscles capable of movement: Hip flexor muscles (e.g., iliopsoas muscles) ⇒ Hip flexion
The hip joint can be flexed, but the knee joint bends unintentionally, resulting in knee fracture.
Therefore, it is necessary to use a long leg brace + a two-handed cane, but it is possible to walk. However, considering durability and safety, it is at the level of a wheelchair.
L3
Typical muscles capable of movement: quadriceps ⇒ hip flexion, knee extension
The quadriceps muscle, which is the knee joint extensor muscle, is effective, so the patient has acquired considerable walking and mobility ability. However, instability of the lower leg and ankle joints is present, so a short leg orthosis (often with a metal brace) is necessary.
Knee stability and lower limb clearance are improved, allowing patients to use stairs and escalators.
L4, L5 and below
Typical muscles that can be operated: lower leg muscle group (mainly peroneal nerve area) => ankle dorsiflexion
Almost the same function as L3. However, while L3 patients were fitted with short leg orthoses with metal supports, simple and lightweight orthoses such as plastic orthoses and orthopses are often sufficient for L4-5 patients. There are also many patients who can walk without a cane.
S1 and below
This is the only area that is not often damaged. If there is, it is due to a car accident or cauda equina tumor. Basically, there are no ADL problems except for urination and defecation. Unfortunately, urination and defecation are S4-5, the true terminal functions, so a spinal cord injury does not mean that the patient is unscathed.
As you can see, the functions and movements possible with a spinal cord injury vary greatly depending on the height of the injury.
It would be difficult to remember them all, so it would be better to remember the muscles that move at each height and think about the function of those muscles.
One height can change the world.
I have briefly mentioned the important points. For more details, please refer to the official book.
That is all. Please come back again.
